If lansoprazole feels wrong, it does not automatically mean the drug is failing. Timing, dose, rebound acid, meal pattern, and non-acid triggers can all distort the picture. The important point is not to stop a proton pump inhibitor abruptly on your own. A step-down conversation and symptom review usually makes more sense than guessing from one rough week.
How we evaluated lansoprazole step-down support
We prioritized deprescribing guidance from this PMC review on proton pump inhibitor deprescribing, practical symptom guidance from the Mayo Clinic GERD overview, and Cleveland Clinic information on acid reflux and GERD. We compared symptom pattern, timing, and step-down practicality rather than promising that one supplement can replace a prescription. We excluded abrupt-stop advice because rebound acid is common and muddies the interpretation fast.
Why can lansoprazole feel wrong even when it is partly helping?
Lansoprazole lowers gastric acid production, but symptom relief still depends on the real driver of the discomfort. If the main issue is meal size, late-night eating, regurgitation, aerophagia, stress-amplified sensitivity, or non-acid reflux, a PPI may help only part of the picture. The Mayo Clinic and Cleveland Clinic both emphasize that reflux symptoms vary and are not always identical from person to person. Timing matters too. A PPI taken inconsistently or at the wrong time relative to meals can feel weaker than it actually is. Some people also interpret new bloating, burping, or nausea as proof the medication is wrong, when the real issue is that the original reflux problem is mixed with eating pattern or upper-gut motility issues. One rough week rarely gives a clean answer by itself.
What signs suggest timing, dose, or rebound instead of true medication failure?
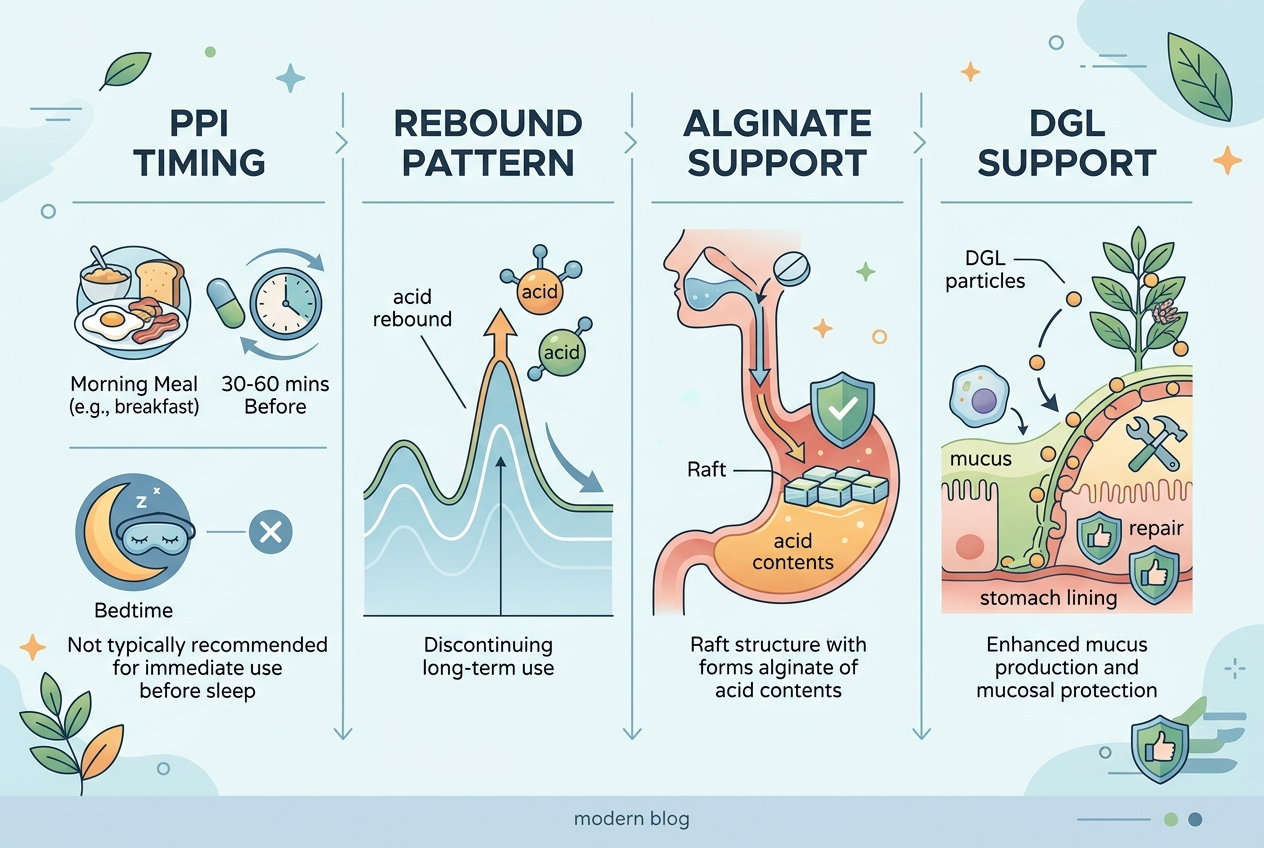
Pattern changes are the biggest clue. If symptoms improved at first and then surged after missed doses, spacing doses, or stopping quickly, rebound acid becomes more plausible. The PMC deprescribing review notes that stopping PPIs can produce rebound symptoms that mimic the return of the original problem. If symptoms mainly flare after late meals, coffee, alcohol, or lying flat, the medication may be under-supported by routine rather than inherently wrong. If symptoms are mostly sour taste, throat burn, or post-meal regurgitation, that still fits reflux logic. If the pattern is severe swallowing trouble, vomiting, bleeding, or progressive pain, that is not a supplement problem. That is a medical-review problem. Dose timing matters too. PPIs usually work best when taken consistently before meals, not randomly after symptoms are already loud. A messy routine can make a reasonable medication look ineffective.
Which daily support options make the most sense during a step-down conversation?
Some links below are affiliate links. This does not influence our evaluation criteria or recommendations.
| Option | Main role | Best fit | Main watch-out |
|---|---|---|---|
| Yuve DGL Licorice | Demulcent-style upper-GI soothing support | People building a gentler daily routine while discussing step-down options | Does not replace prescription management |
| Yuve DGL Licorice Chewables | Chewable upper-GI support before or after trigger meals | People who want a portable routine format | Still needs timing consistency to judge fairly |
| Gaviscon Advance | Alginate barrier support above stomach contents | People whose pattern includes regurgitation after meals or lying down | Works differently from a PPI and may need repeat use |
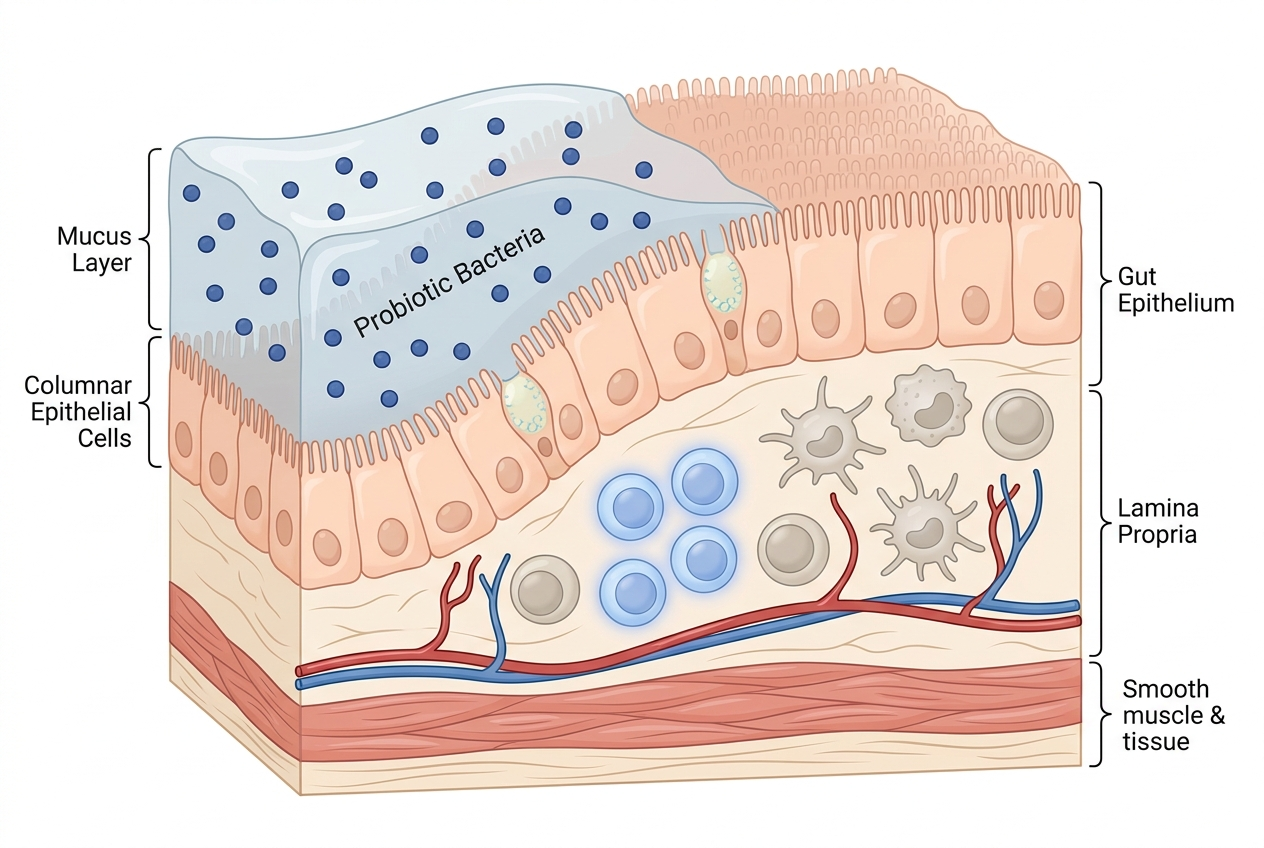
| Yuve Probiotic Gummies | Routine gut-balance support when bloating or irregularity is part of the picture | People with mixed upper-gut and lower-gut symptoms | Not a direct acid-control tool |
A step-down support tool should match the symptom pattern, not pretend to be the same thing as a PPI.
When should you seek review instead of experimenting longer?
If swallowing feels harder, food sticks, vomiting persists, blood appears, weight drops unintentionally, chest pain is severe, or symptoms escalate despite a consistent plan, it is time for medical review. Those are not normal “maybe this med is not for me” signals. They are escalation signals. The Mayo Clinic lists swallowing difficulty and weight loss as reasons to get evaluated. This matters even more if you are changing a prescription. A smart routine can still help. Smaller dinners, earlier eating, fewer trigger foods at night, and a cleaner symptom log all improve the conversation. But the role of daily support is to make the pattern easier to read, not to delay proper care. The goal is clarity and steadiness, not cowboy medication changes.
FAQ
Does more bloating on lansoprazole prove it is the wrong medication?
No. Bloating can reflect meal pattern, swallowed air, constipation, or the original reflux pattern itself. One symptom does not settle the whole question.
Can you stop lansoprazole suddenly if you feel worse?
That is usually a bad idea without medical guidance. The PMC deprescribing review notes that rebound acid can make a quick stop feel worse than the baseline problem.
What kind of support makes sense during a step-down?
That depends on the pattern. Alginate-style options fit regurgitation patterns, while DGL-style support may fit people building a gentler upper-GI routine around meals.
Are probiotics a direct replacement for PPIs?
No. Probiotics can support routine gut balance, but they do not perform the same acid-lowering function as a proton pump inhibitor. Different mechanisms, different job.
What is the cleanest way to judge whether lansoprazole is helping?
Keep dose timing, meal timing, and bedtime consistent for several days while logging symptoms. Clean routines produce clearer answers than random changes.
When is the pattern too risky for self-testing?
If symptoms include bleeding, progressive swallowing trouble, severe chest pain, or unexplained weight loss, stop experimenting and get checked. Those signals deserve real review.