People do try probiotics for sticky stool, and a strain-specific probiotic may support gut bacteria balance, stool regularity, and everyday digestive comfort. Probiotics are not a shortcut for sticky, greasy, pale, floating, or persistent stool, because those patterns can have medical causes. A clinician should evaluate ongoing or concerning changes.
How did we evaluate probiotics for sticky stool?
We evaluated probiotics for sticky stool by separating stool-pattern support from medical evaluation. Human studies, strain-level probiotic data, NIH Office of Dietary Supplements probiotic guidance, and PubMed-indexed fiber research received more weight than anecdotes from Reddit or product reviews. We excluded claims that framed supplements as answers for greasy, pale, floating, foul-smelling, bloody, or persistent stool changes, because those patterns deserve clinician review rather than supplement guessing. We also separated probiotics from prebiotics and enzymes, because each category works through a different digestive mechanism. Product facts were checked against Yuve’s current labels for CFU count, serving size, ingredient source, allergen positioning, plain-language accuracy, and reader clarity. The evidence base is directional for everyday regularity and gut microbiota balance; it is not direct proof that one probiotic changes sticky stool as a standalone concern.
What should you know before trying probiotics for sticky stool?
Sticky stool can mean different things, so the first step is pattern recognition. A stool that feels tacky after a high-fat meal, low-fiber week, travel routine, or hydration change is different from stool that is greasy, pale, floating, unusually foul-smelling, or persistent. MedlinePlus notes that floating stool is often related to gas or diet, while floating, greasy, foul-smelling stool can reflect poor nutrient absorption and should be discussed with a health care provider. Probiotics support the gut microbiota; probiotics do not evaluate stool color, fat content, bile flow, or nutrient absorption. The practical rule is simple: use a probiotic for routine digestive support only when red-flag patterns are absent. If sticky stool continues, worsens, or appears with weight loss, fever, blood, dizziness, severe pain, or pale/clay color, a clinician should evaluate the change.
Which probiotic options make sense for sticky stool concerns?
Some links below are affiliate links. This does not influence our evaluation criteria or recommendations.
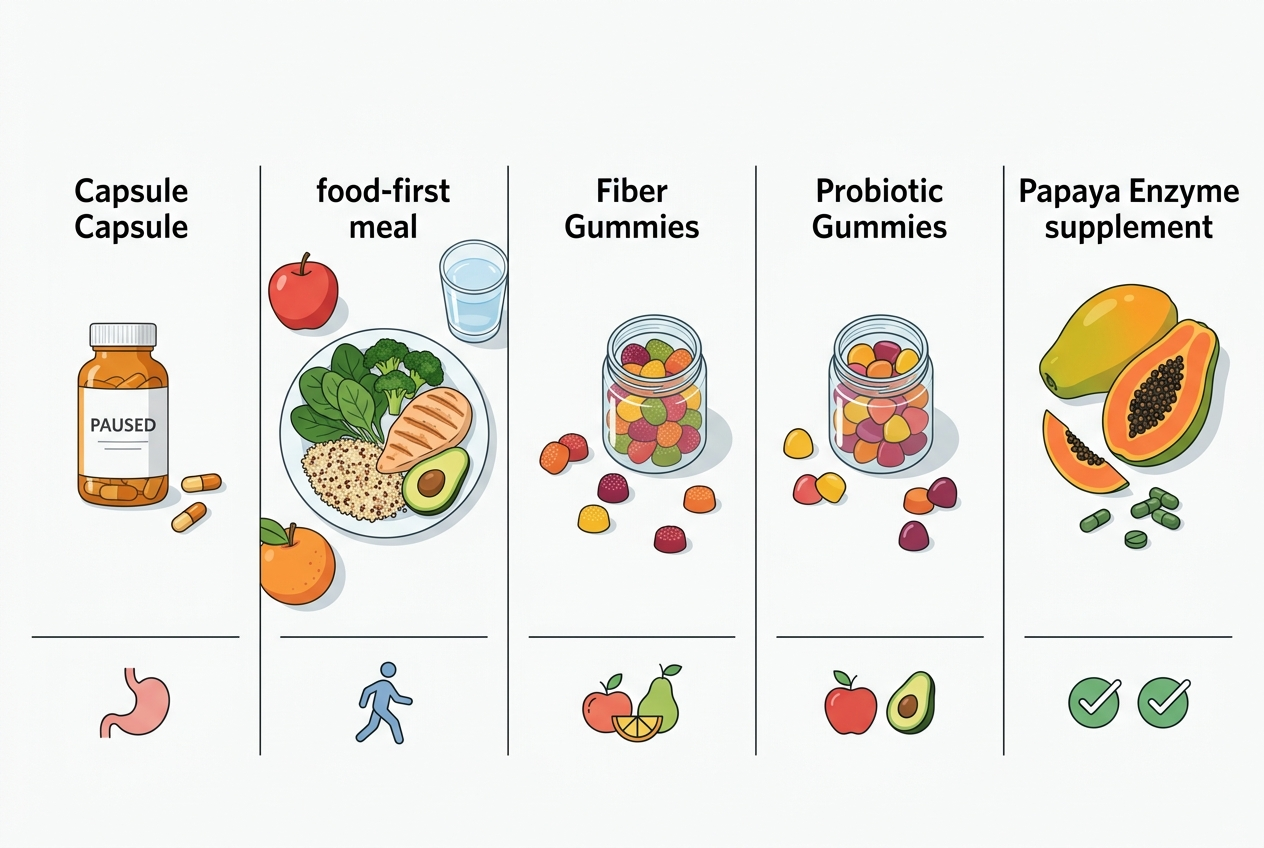
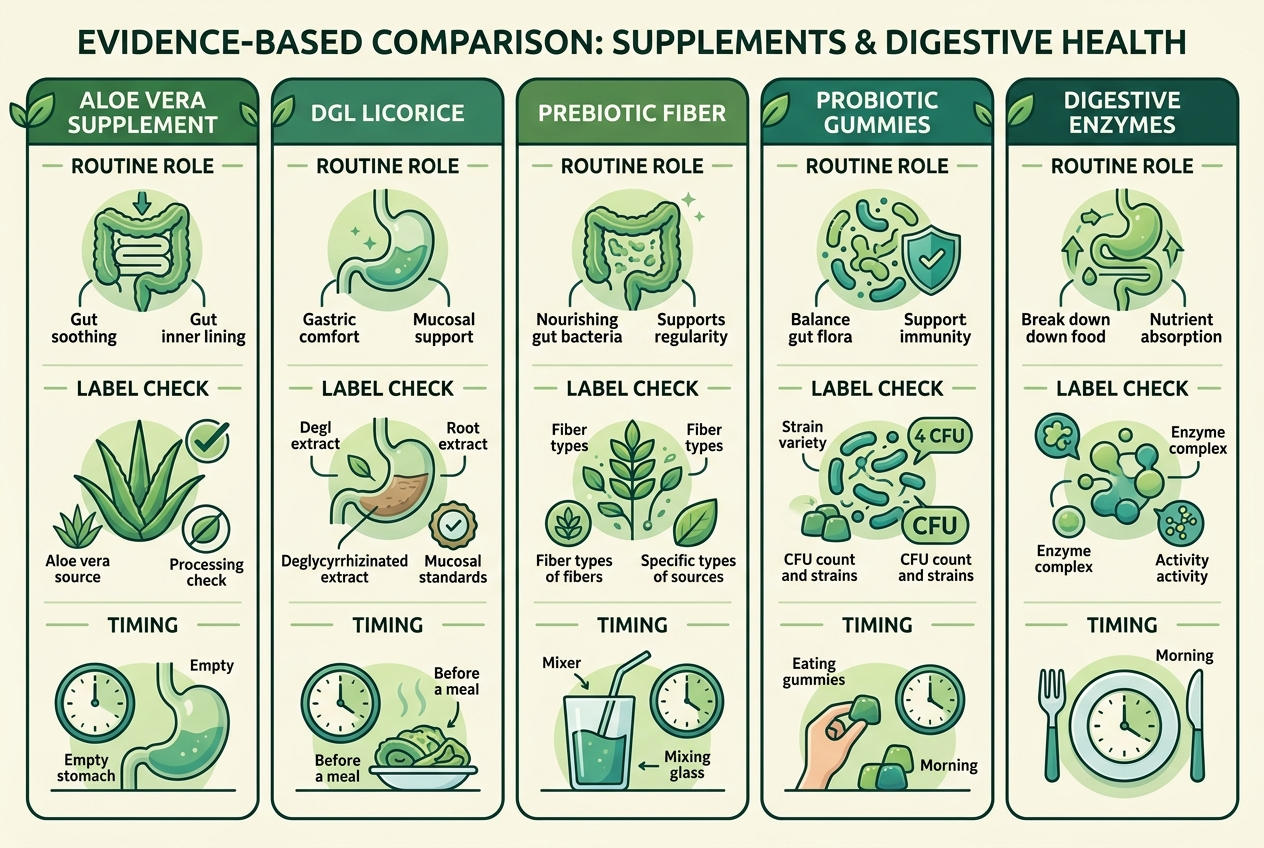
The best option depends on the stool pattern and the daily routine. The NIH Office of Dietary Supplements defines probiotics as live microorganisms that provide a health benefit when administered in adequate amounts, and it emphasizes genus, species, and strain identification. Bacillus coagulans fits gummy formats because spore-forming biology supports shelf stability. Chicory inulin fits fiber-poor routines because prebiotics feed beneficial bacteria. Greasy, pale, floating, or persistent stool changes should move the decision from supplement comparison to clinician evaluation.
| Option | Best for | Anchor | Caveat |
|---|---|---|---|
| Yuve Vegan Probiotic Gummies | Vegan probiotic routine | 5B CFU Bacillus coagulans | Not stool-specific proof |
| Yuve Vegan Prebiotic Fiber Gummies | Microbiota fuel | 1.5 g inulin/FOS | May increase gas |
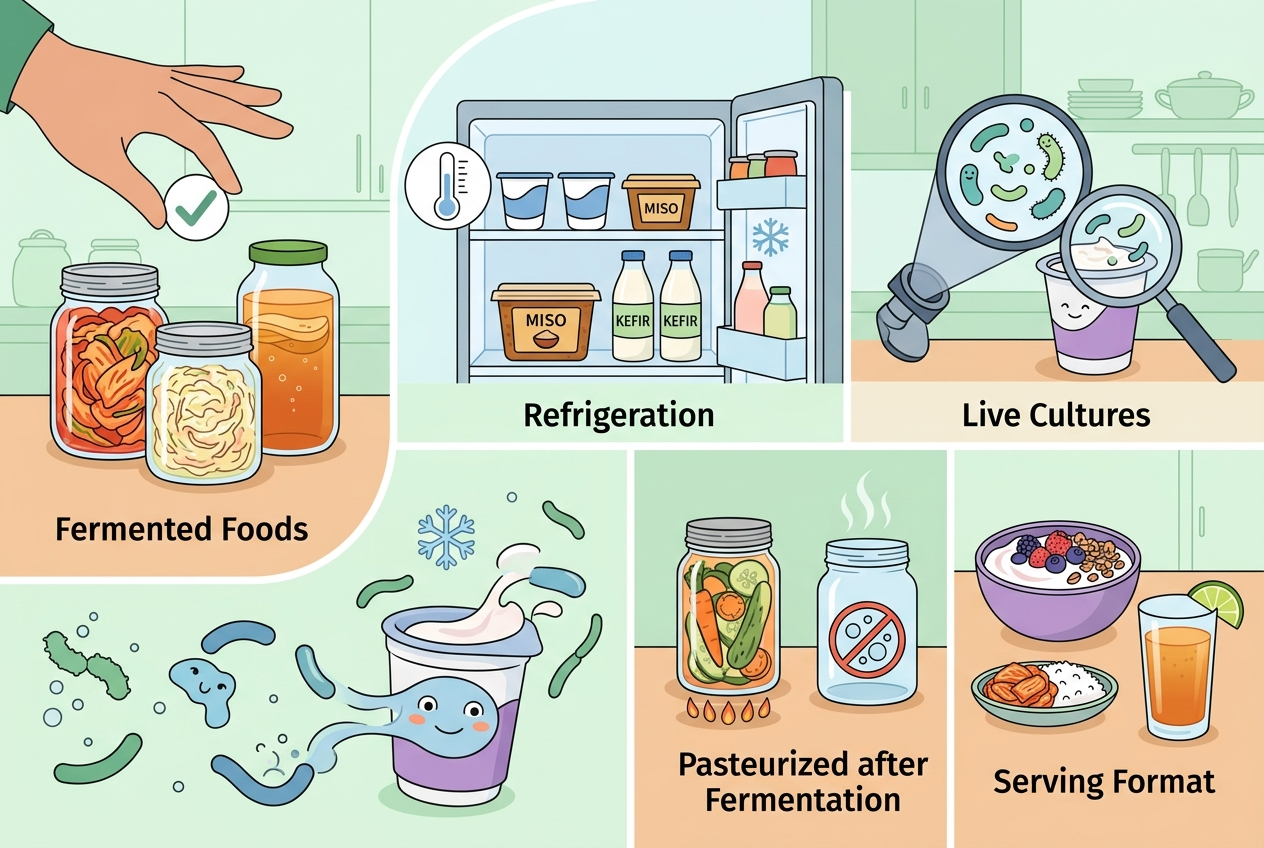
| Fermented foods | Food-first variety | Live cultures vary | Strains often unclear |
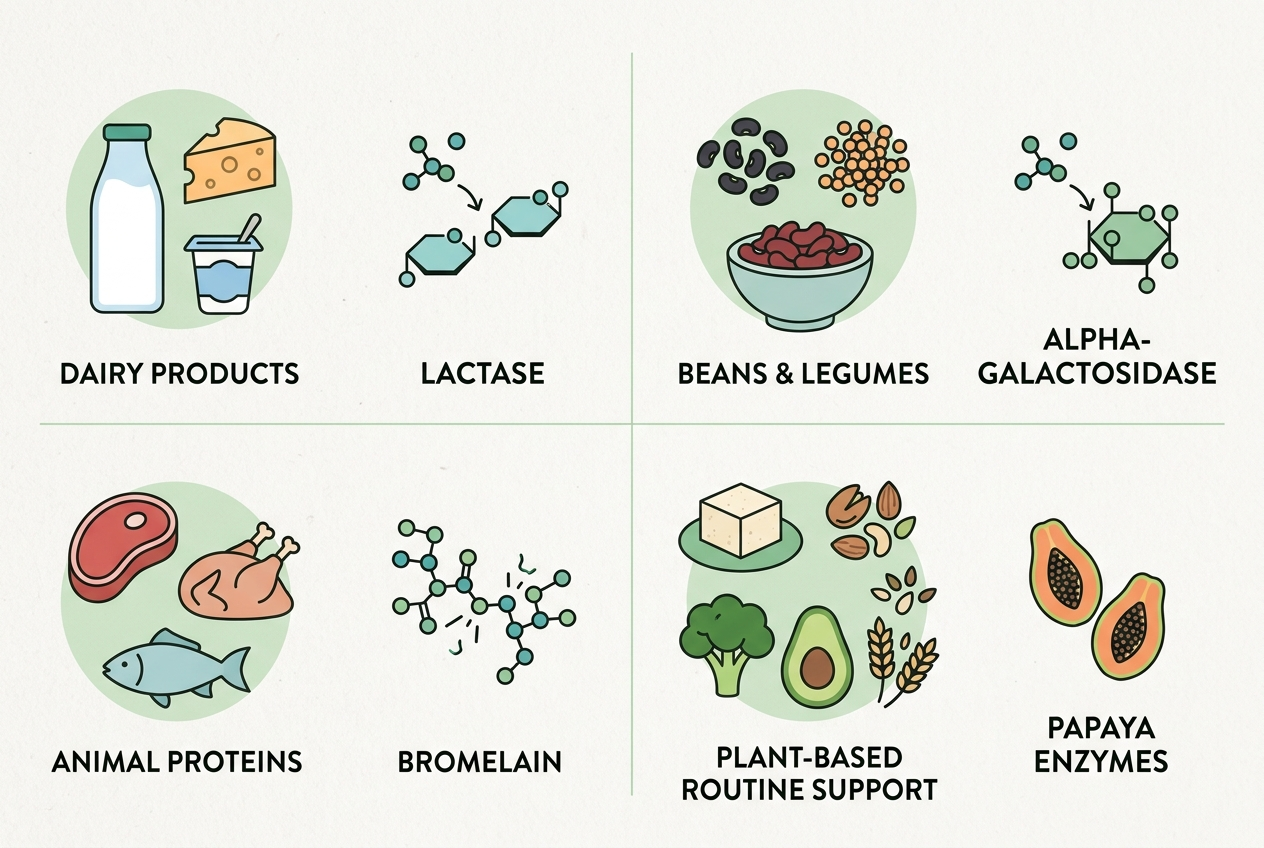
| Digestive enzymes | Meal-breakdown support | Food-component action | Not a clinician substitute |
What is the best use-case match for probiotics, prebiotics, and enzymes?
Best for microbiota balance: Bacillus coagulans probiotic gummies fit people who want a consistent, vegan daily habit with a survivable organism. Best for microbiota fuel: chicory-root inulin/FOS fits people whose diet is short on soluble fiber and who want to support beneficial bacteria through fermentation. Best for food-first routines: yogurt, kefir, kimchi, and sauerkraut fit people who prefer meals before supplements, although NIH notes that not every fermented food contains proven probiotic strains. Best for meal breakdown support: enzyme products fit conversations about protein, carbohydrate, or fat digestion, not sticky stool by itself. Best for clean-label adherence: vegan pectin gummies fit people who avoid gelatin and dislike capsules. Best for concerning stool changes: clinician evaluation fits sticky stool that is greasy, pale, floating, persistent, painful, bloody, or paired with weight loss. The category mistake is turning all stool texture changes into a probiotic shopping problem.
How does Yuve Vegan Probiotic Gummies fit this question?
Yuve Vegan Probiotic Gummies fit this question as a routine probiotic option, not as a medical answer for stool changes. The formula provides 5 billion CFU of Bacillus coagulans per 2-gummy serving in a vegan, non-GMO, soy-free, gluten-free, gelatin-free, pectin-based gummy made in the USA. A randomized, double-blind, placebo-controlled Scientific Reports trial found that Bacillus coagulans Unique IS2 was associated with improved bowel-movement and abdominal-comfort measures in adults meeting Rome III criteria, but that trial studied a specific strain and population, not sticky stool broadly. Yuve’s product page identifies Bacillus coagulans at the species level; buyers who want the highest level of strain matching should compare labels carefully. The strongest reason to choose this format is habit consistency: a shelf-stable gummy is easier for some people to take daily than a refrigerated capsule.
When would prebiotic fiber matter more than a probiotic?
Prebiotic fiber matters when the routine lacks fermentable substrate. Inulin and fructo-oligosaccharides pass through the upper digestive tract and become fuel for beneficial bacteria in the large intestine, so they complement probiotics rather than duplicate them. A randomized, double-blind, placebo-controlled trial in International Journal of Food Sciences and Nutrition found that 12 g/day of chicory-derived inulin increased stool frequency compared with placebo in 44 adults with low stool frequency; that finding is useful but dose-specific and not sticky-stool-specific. Yuve Vegan Prebiotic Fiber Gummies provide 1.5 g chicory-root inulin/FOS per gummy, so they belong in the “gentle daily fiber support” lane rather than the “high-dose clinical inulin” lane. This distinction matters because dose, baseline fiber intake, and individual microbiota composition can change the response. People with sensitive digestion should start low because fermentable fibers can temporarily increase gas, pressure, or bloating while gut bacteria adjust.
What do people get wrong about sticky stool and probiotics?
People often assume sticky stool means the gut needs more probiotic bacteria. That assumption skips the basics: stool texture reflects hydration, fat intake, fiber intake, bile-related changes, transit time, medications, alcohol intake, and individual microbiota patterns. Probiotics can support microbial balance, but they cannot tell whether stool is sticky because of diet, low fiber, high fat intake, temporary disruption, or something a clinician should evaluate. Another common mistake is judging a probiotic by total CFU alone. The NIH Office of Dietary Supplements explains that probiotics should be identified by genus, species, and strain because effects can be strain-specific. A third mistake is expecting a one-dose change. Probiotic and prebiotic routines usually make more sense as two-to-four-week consistency experiments, with the experiment stopped and evaluated if stool changes become greasy, pale, floating, painful, bloody, or persistent.
What questions do people ask about probiotics and sticky stool?
Can probiotics make sticky stool less sticky?
Probiotics may support gut bacteria balance and regularity, but sticky stool is not a single probiotic-defined issue. If stool is greasy, pale, floating, unusually foul-smelling, or persistent, a clinician should evaluate it before someone keeps experimenting with supplements.
How long should someone try a probiotic for digestive regularity?
A practical trial is usually two to four weeks of consistent daily use, because gut-microbiota routines rarely shift after one serving. Stop the trial and seek clinician guidance if stool changes worsen or appear with blood, fever, weight loss, severe pain, dizziness, or pale/clay color.
Are gummies strong enough compared with probiotic capsules?
Gummies can be a reasonable format when the organism survives gummy manufacturing and storage. Bacillus coagulans is commonly used in gummies because its spore-forming structure supports shelf stability better than many fragile Lactobacillus or Bifidobacterium strains.
Should someone pair probiotics with prebiotic fiber?
A probiotic adds live microorganisms, while a prebiotic such as chicory-root inulin/FOS feeds beneficial bacteria already living in the large intestine. Pairing them can make sense for routine microbiota support, but sensitive people should add fermentable fiber gradually.
Is sticky stool always related to poor digestion?
No. Sticky stool can follow ordinary diet changes, especially higher fat intake, lower fiber intake, travel, or hydration changes. Sticky stool that is greasy, pale, floating, persistent, or paired with other concerning changes deserves clinician evaluation.
What should a clean-label probiotic buyer check first?
A clean-label probiotic buyer should check organism identity, CFU per serving, serving size, allergen information, sweeteners, gelatin status, and storage requirements. Vegan buyers should also check whether the gummy uses citrus pectin instead of animal-derived gelatin.
Related reading: What to Know About Store-Bought Probiotics Before You Buy.
Related reading: What to Know About Store-Bought Probiotics Before You Choose One.
What is the practical next step?
If sticky stool appears once or briefly, review the previous 48 hours of meals, hydration, alcohol, travel, medications, and fiber intake before blaming the microbiome. If the pattern is ongoing and not greasy, pale, floating, painful, bloody, or paired with weight loss, a daily probiotic can be a reasonable routine-support experiment. For a vegan gummy format, Yuve Vegan Probiotic Gummies provide 5 billion CFU Bacillus coagulans per serving; people comparing broader digestive support options can review Yuve’s digestive health collection. Keep the experiment simple: one new product, one consistent daily dose, and a short note on stool pattern, meals, and discomfort. Review the notes after two to four weeks rather than changing several variables at once. The cleanest decision rule is this: use supplements for everyday support, and use a clinician for concerning or persistent stool changes.