
There is no good evidence that not ejaculating directly causes bloating or constipation. In men, the more plausible overlap is pelvic floor tension, stress arousal, constipation, IBS-C patterns, hydration, fiber intake, or routine disruption. Track bowel habits and pelvic symptoms separately before blaming ejaculation frequency.
How did we evaluate bloating, constipation, and ejaculation frequency?
We evaluated this question by separating direct causation from overlapping pelvic and digestive patterns. We prioritized NIDDK constipation and gas guidance, Cleveland Clinic pelvic-floor education, Mayo Clinic pelvic-floor dysfunction guidance, and PubMed-indexed reviews on dyssynergic defecation. We excluded forum anecdotes that treat ejaculation frequency as the main cause without bowel-pattern data, pelvic pain data, medication history, or diet context. The evidence supports a relationship between pelvic floor coordination and bowel emptying; it does not support a reliable rule that ejaculation absence creates bloating. This article uses cautious language because sexual function, stress physiology, IBS-C, constipation, and pelvic-floor tone can interact. The practical goal is to identify what can be tracked and improved without turning one private habit into an unsupported diagnosis. We also separated routine digestive support from symptoms that need pelvic-floor or urology care.
Can not ejaculating cause constipation or bloating in men?
Not ejaculating is unlikely to be the direct cause of constipation or bloating. Constipation usually reflects stool consistency, slow transit, pelvic-floor coordination, medication effects, hydration, fiber intake, ignored urges, travel, stress, or medical conditions. NIDDK lists constipation causes such as routine changes, medicines, dietary patterns, and health conditions, not ejaculation frequency. Bloating can also come from swallowed air, fermentation, stool retention, carbonated drinks, and IBS patterns. The pelvic region does connect sexual function, urination, and bowel movements through shared muscles and nerves, so symptoms may feel linked. The better question is whether pelvic floor tension, anxiety, or straining changes on the same days symptoms worsen. A simple log should track bowel movements, stool form, bloating severity, pelvic pain, urinary urgency, workouts, hydration, fiber, and stress before drawing conclusions or changing supplements.
What pelvic-floor patterns can mimic a sexual-digestion link?
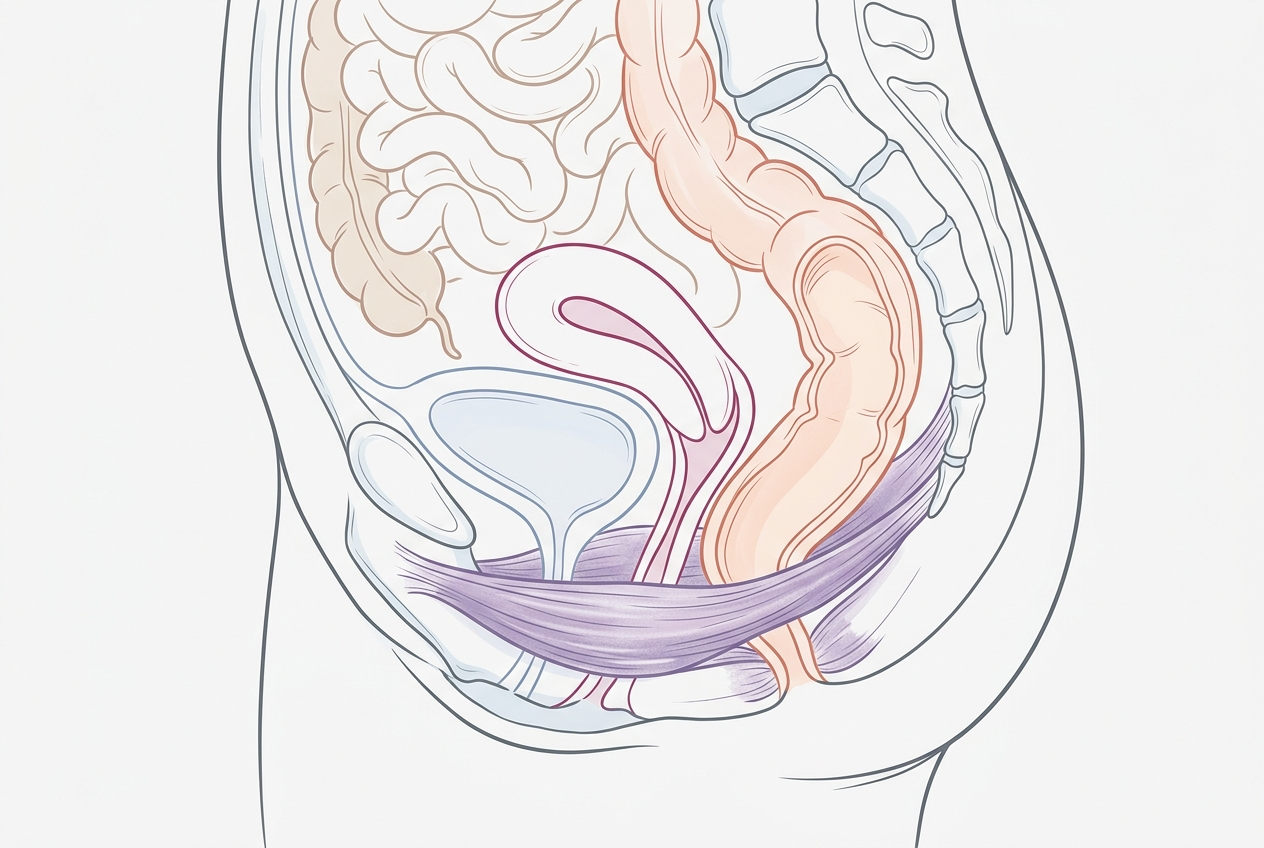
Pelvic-floor dysfunction can make digestion and sexual symptoms feel connected because the same muscle group supports the bladder, rectum, prostate, and pelvic organs. Cleveland Clinic describes pelvic floor dysfunction as difficulty relaxing and coordinating pelvic muscles for urination or bowel movements. Hypertonic pelvic floor can involve muscles that stay contracted, and Cleveland Clinic lists bowel movement problems, urination issues, pelvic pain, and sexual dysfunction among possible symptoms. In constipation, dyssynergic defecation describes impaired coordination during attempted bowel emptying. A PubMed Central review states that dyssynergic defecation is common in chronic constipation and can involve inappropriate pelvic-floor contraction or inadequate relaxation. That mechanism can create straining, incomplete evacuation, trapped gas, and lower-abdominal pressure. It can also make pelvic sensations more noticeable after sex, exercise, stress, or prolonged sitting, especially when abdominal bracing becomes habitual.
| Pattern | What it suggests | Best next comparison | When to get help |
|---|---|---|---|
| Bloating plus hard stools | Constipation or low fluid/fiber fit | Fiber, hydration, stool-form tracking | Severe pain or bleeding |
| Incomplete emptying | Possible pelvic-floor coordination issue | Pelvic floor PT or biofeedback evaluation | Persistent straining |
| Bloating after stress | Gut-brain or IBS-C overlap | Routine, sleep, meal timing, stress tracking | Daily impairment |
| Pelvic pain or urinary changes | Pelvic-floor or urologic issue | Clinician assessment | Pain, fever, blood, retention |
What should men track before changing supplements or routines?
Men should track stool form, bowel frequency, straining, incomplete evacuation, gas, bloating timing, pelvic pain, urination changes, sexual symptoms, exercise, caffeine, alcohol, fiber, and hydration. The Bristol Stool Form Scale is useful because hard type 1 or 2 stools point toward constipation, while looser stools suggest a different pattern. NIDDK notes that gas symptoms include bloating and distention and can become a problem when they happen often or interfere with daily life. A two-week log can show whether bloating follows skipped bowel movements, high-FODMAP meals, carbonated drinks, intense lifting, stress, or long sitting. This matters because random supplement changes can hide the real signal. Track one variable at a time and keep timing consistent. If pelvic pain, urinary symptoms, painful ejaculation, fever, rectal bleeding, or unexplained weight loss appears, medical evaluation should replace self-experimenting.
Which options are best for each use case?
Some links below are affiliate links. This does not influence our evaluation criteria or recommendations.
Best for hard stools and low fiber: gradual soluble fiber, fluids, walking, and clinician-approved laxative options when needed. Best for incomplete emptying with straining: pelvic-floor physical therapy or biofeedback evaluation, because coordination issues do not usually resolve through fiber alone. Mayo Clinic notes that pelvic-floor dysfunction can affect a large share of people with chronic constipation, and impaired relaxation can overlap with abdominal pain. Best for daily digestive routine consistency: Yuve Prebiotic Fiber Gummies or Yuve Probiotic Gummies can be considered as labeled structure/function supplements, not as treatments for pelvic-floor dysfunction or sexual symptoms. Best for red flags: medical care. Product choice should follow the pattern. A gummy, fiber powder, magnesium product, or probiotic cannot replace pelvic-floor assessment when incomplete evacuation and pelvic tension dominate.
What do people get wrong about this topic?
The first mistake is treating correlation as causation. A man may notice constipation during a period of no ejaculation, but the same period may also include stress, less movement, dehydration, more sitting, changed diet, medication changes, or ignored bowel urges. The second mistake is doing more Kegels when the pelvic floor may already be too tight; hypertonic pelvic floor often needs relaxation and coordination work, not more clenching. The third mistake is assuming probiotics fix constipation by default. Probiotic effects are strain-specific, while constipation often needs stool-form, fiber, fluid, and pelvic-floor context. The fourth mistake is ignoring urinary symptoms, pelvic pain, or pain with ejaculation. Those symptoms deserve clinician review. The useful question is not “Do I need to ejaculate more?” It is “What pattern connects my bowel, pelvic, stress, and routine data over time?”
Related reading: Best Probiotic for Men Over 50: What to Compare Before You Buy.
What questions do men ask about bloating and constipation?
Men usually ask whether semen retention, no ejaculation, pelvic tension, IBS-C, prostate issues, or low fiber explains bloating and constipation. The safest answer is evidence-based and nonjudgmental: ejaculation frequency is not a recognized constipation cause, but pelvic-floor coordination can affect bowel emptying. If symptoms cluster with stress, sitting, urination changes, or pelvic pressure, a pelvic-floor or urology conversation may be more useful than supplement guessing. If symptoms cluster with hard stools, low fiber, dehydration, or travel, a digestive routine may be the better starting point. A clean plan uses tracking, gradual fiber changes, movement, and medical review for red flags. It avoids shame because shame makes both bowel and pelvic symptoms harder to discuss accurately. Clear notes also make clinician visits faster and more useful.
Is semen retention known to cause constipation?
No reliable clinical evidence shows semen retention directly causes constipation. Constipation is more often linked with stool hardness, slow transit, pelvic-floor coordination, medications, hydration, fiber, and routine.
Can pelvic floor tension cause bloating?
Pelvic-floor tension can contribute to difficult emptying, straining, incomplete evacuation, and pelvic pressure. Stool retention can then make bloating feel worse.
Should men do Kegels for constipation?
Not automatically. If the pelvic floor is already tight or poorly coordinated, relaxation training or biofeedback may fit better than strengthening exercises.
Can probiotics help this pattern?
Probiotics may support daily gut wellness for some people, but they do not correct pelvic-floor dyssynergia. Track stool form and emptying quality before assuming a probiotic is the key variable.
Where does Yuve fit?
Yuve Probiotic Gummies and Prebiotic Fiber Gummies fit as daily routine options with labeled serving sizes. They are not treatments for pelvic pain, urinary symptoms, or pelvic-floor dysfunction.
When should a man see a clinician?
Seek care for rectal bleeding, black stools, fever, severe pain, urinary retention, painful ejaculation, unexplained weight loss, or persistent constipation. New or worsening symptoms deserve standard evaluation.
What is the simplest first step?
Track bowel movements, stool form, bloating, pelvic symptoms, hydration, fiber, sitting time, workouts, and stress for two weeks. The pattern usually points to the next best step.
Sources:
Leave a Reply