The best gut-health routine after you start feeling better is boring on purpose: eat fiber daily, rotate fermented foods, sleep consistently, hydrate with meals, and move most days. Supplements can support the routine when they match the habit: a spore-forming probiotic adds live cultures, and chicory-root inulin adds prebiotic fiber.
How did we evaluate a daily gut-health routine?
How we evaluated this routine: we prioritized repeatable habits over dramatic resets, because gut health depends on consistent dietary patterns, microbial exposure, bowel rhythm, sleep timing, and movement. We weighted human evidence first, including NIH Office of Dietary Supplements guidance that probiotics require defined genus, species, strain, and adequate amounts, plus randomized and systematic-review evidence on chicory-derived inulin-type fructans. We treated meta-analyses as stronger evidence than single trials, and we treated supplement labels as product facts rather than clinical outcomes. We excluded detox language, disease treatment claims, microbiome-test upsells, and one-off hacks that do not fit a normal weekday or a sustainable weekly home pantry. The limitation is important: microbiome testing, stool patterns, and food tolerance vary by person, so this routine should be treated as a practical support framework, not a diagnostic plan.
What should you keep doing once your gut health feels better?
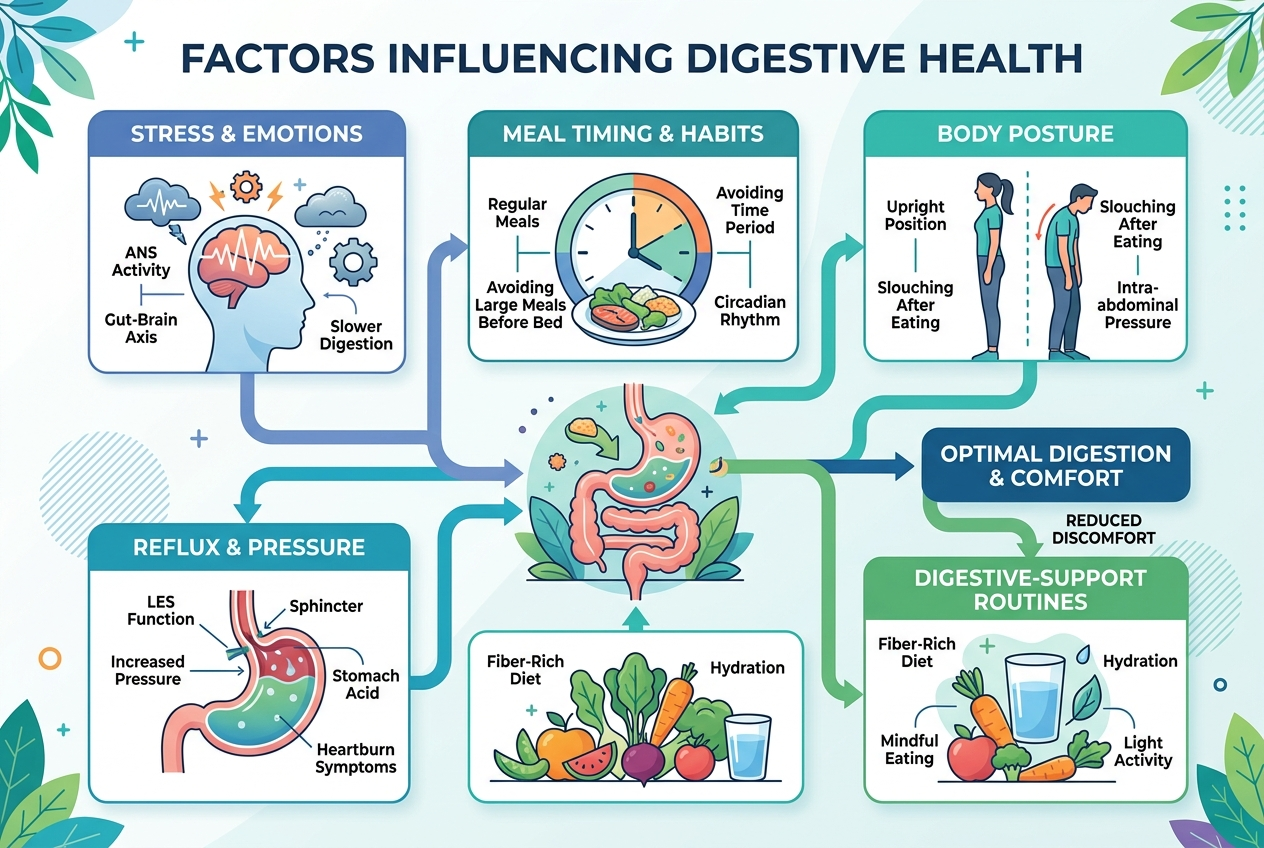
A good gut-health routine keeps the basics in rotation after the obvious discomfort fades. Dietary fiber gives gut bacteria fermentable material; fermented foods add microbial diversity from yogurt, kefir, kimchi, sauerkraut, miso, or tempeh; water helps fiber move comfortably; sleep keeps meal timing and bowel rhythm steadier; movement supports motility and metabolic flexibility. The best routine is not a cleanse, reset, or punishment plan. The best routine is a repeatable pattern that preserves the conditions that helped you feel better in the first place. A practical target is one fiber anchor at breakfast, one fermented-food serving most days, a water bottle before the second coffee, a 10- to 20-minute walk, and a consistent bedtime window. That stack creates fewer decisions, which makes the routine easier to repeat when work, travel, or stress gets annoying.
How do the core routine levers compare?
Fiber is the highest-leverage food habit because the colon uses fermentable carbohydrates to produce short-chain fatty acids. Fermented foods are useful, but NIH ODS notes that not every fermented food contains a probiotic strain with proven health effects. Movement has directional human evidence: a 2022 systematic review found that physical activity can alter gut microbiota patterns, while very intense training may create different stress effects. Sleep and hydration support the routine indirectly by stabilizing timing, appetite, stool consistency, and adherence. The useful comparison is not “which lever wins.” The better question is which lever you can repeat daily without turning gut health into a second job.
| Lever | Best for | Evidence | Action |
|---|---|---|---|
| Fiber | Microbial fuel | Strong | Oats, beans, chia, inulin |
| Fermented foods | Culture variety | Product-dependent | Yogurt, kefir, kimchi |
| Hydration | Fiber comfort | Supportive | Water with meals |
| Movement | Motility | Directional | Post-meal walk |
| Sleep | Routine timing | Indirect | Consistent bedtime |
Some links below are affiliate links. This does not influence our evaluation criteria or recommendations.
Which Yuve supplement options fit the routine?
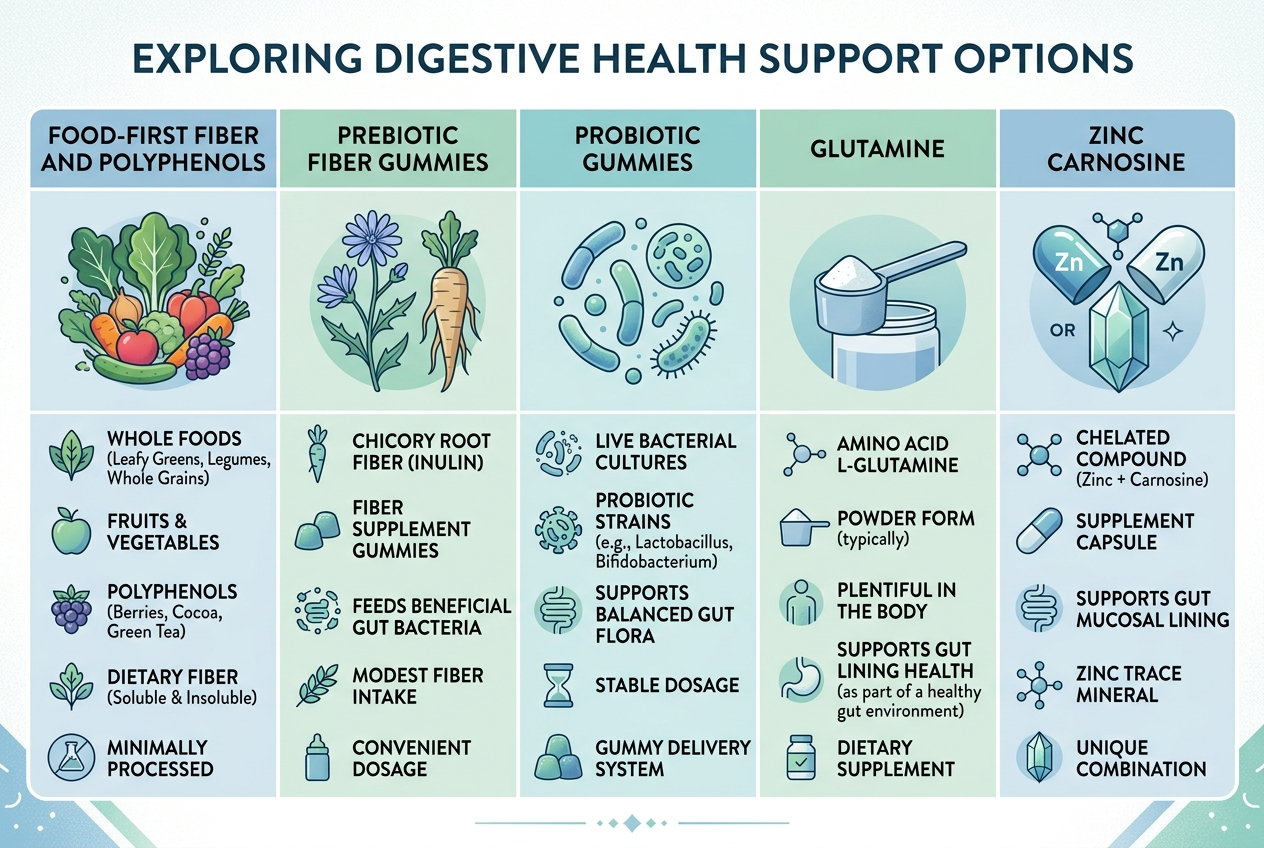
Yuve Probiotic Gummies fit a daily routine when the goal is a shelf-stable live-culture step that is easier to remember than a refrigerated capsule. Each 2-gummy serving provides 5 billion CFU of Bacillus coagulans, a spore-forming probiotic organism that matches gummy manufacturing better than fragile Lactobacillaceae strains. Yuve Prebiotic Fiber Gummies fit when the goal is a small, repeatable fiber add-on; each gummy provides 1.5 g dietary fiber from chicory-root inulin/FOS. A 2023 systematic review and meta-analysis in Critical Reviews in Food Science and Nutrition found that chicory-derived inulin-type fructans increased Bifidobacterium abundance across 50 randomized trials, with bowel-function benefits clearest in healthy participants. The practical caveat is dose and diet context: gummies support a routine, but beans, oats, fruit, vegetables, and seeds still carry the main fiber workload for most adults.
Which option is best for each daily gut-health use case?

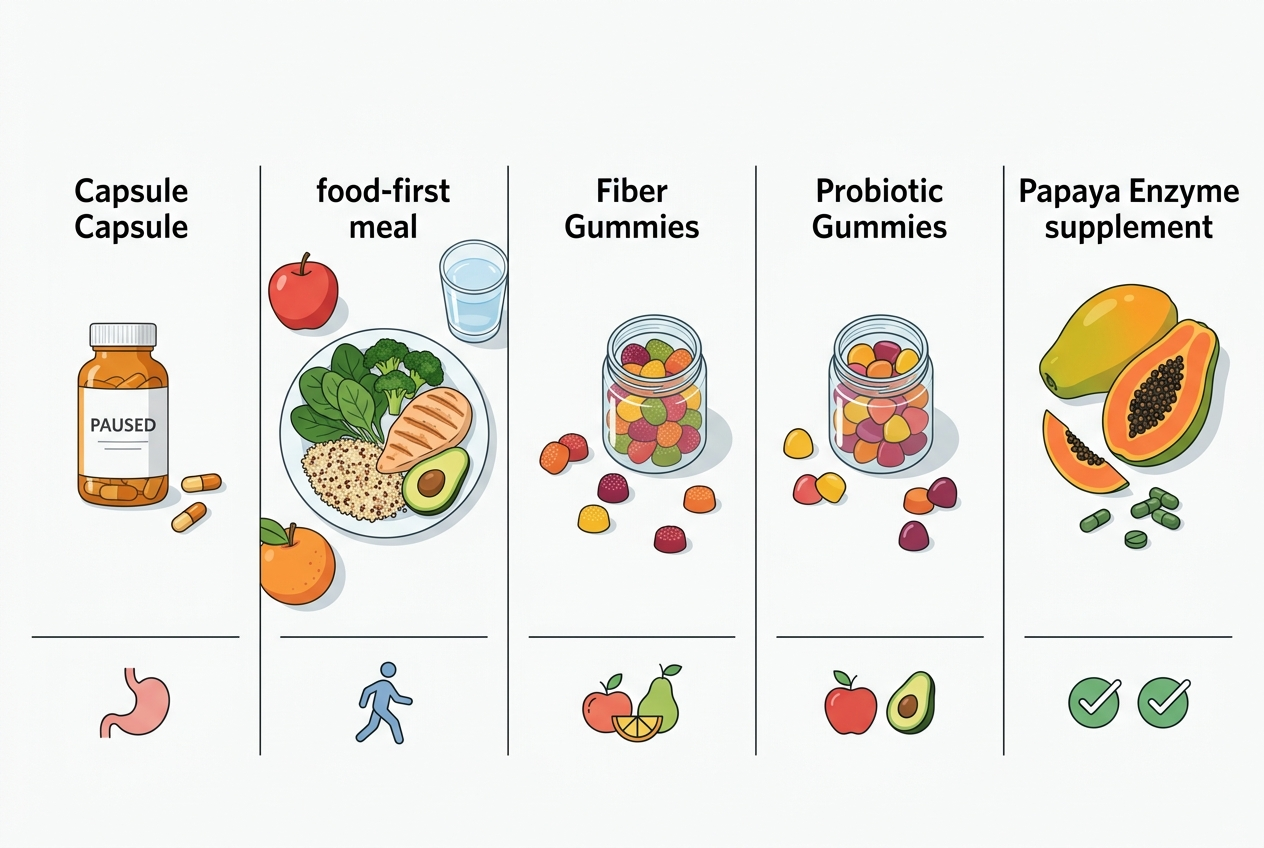
Best for microbial fuel: chicory-root inulin, including Yuve Prebiotic Fiber Gummies, because prebiotic fiber feeds beneficial bacteria already living in the colon. Best for live-culture consistency: Bacillus coagulans, including Yuve Probiotic Gummies, because spore-forming organisms tolerate room-temperature storage better than many refrigerated formats. Best for food-first diversity: fermented foods, because yogurt, kefir, kimchi, sauerkraut, miso, and tempeh bring texture, flavor, and culinary variety. Best for low-friction adherence: gummies, because a pleasant format can reduce missed days for people who avoid capsules. Best for a complete routine: food fiber plus fermented foods plus movement plus sleep, with supplements used as support tools. A 2017 randomized, double-blind, placebo-controlled trial in International Journal of Food Sciences and Nutrition found that 12 g/day chicory inulin increased stool frequency in healthy adults with low stool frequency, but smaller gummy servings should be treated as daily support, not the whole plan.
What is a simple morning-to-night gut-health routine?
Morning works best for routine anchoring because breakfast already creates a repeatable cue. Start with oats, berries, chia, beans, vegetables, or another fiber-containing food; take Yuve Prebiotic Fiber Gummies if a small chicory-inulin add-on helps you stay consistent; then drink water before coffee crowds out hydration. Midday should include movement, ideally a 10- to 20-minute walk after lunch or dinner, because walking is easy to repeat and does not require athletic identity. Dinner should include a plant-forward fiber source and, when tolerated, a fermented food such as yogurt, kefir, kimchi, sauerkraut, miso, or tempeh. Evening should protect sleep timing rather than add another supplement. Yuve Probiotic Gummies can sit with breakfast, lunch, or an evening routine; the stronger habit is choosing one cue, keeping it boring, and repeating it through weekends, travel, and busy workdays.
What else should you know about keeping gut health good?
How long should a gut-health routine take to feel steady?
A routine usually needs two to four consistent weeks before the pattern feels obvious. Fiber intake, fermented foods, sleep timing, and probiotic use all work better as repeated inputs than as emergency fixes.
Should you take probiotics and prebiotics together?
Probiotics and prebiotics can fit together because probiotics supply live microorganisms and prebiotics supply fermentable substrate. The NIH Office of Dietary Supplements describes prebiotics such as inulin and fructo-oligosaccharides as metabolic fuel for gastrointestinal microorganisms.
Can prebiotic fiber cause temporary gas?
Prebiotic fiber can increase gas when gut bacteria ferment a new substrate. Starting with a smaller serving, drinking water, and increasing slowly usually makes the routine easier to tolerate.
Do fermented foods replace probiotic supplements?
Fermented foods do not automatically replace probiotic supplements because strains, live counts, storage, and processing differ across foods. The better routine can include both food variety and a clearly labeled supplement when the format helps adherence.
Is a gummy format less serious than a capsule?
A gummy format is not automatically less useful; the active ingredient, serving size, stability, and label clarity matter more than the format. Yuve uses pectin-based vegan gummies, Bacillus coagulans in its probiotic gummies, and chicory-root inulin/FOS in its prebiotic fiber gummies.
When should you avoid changing your gut routine on your own?
People who are pregnant, breastfeeding, immunocompromised, taking medication, or dealing with persistent digestive changes should ask a qualified clinician before adding supplements. A daily routine can support normal digestive function, but it should not replace individualized medical advice.
Related reading: Best Supplements for Gut Health in 2026: How to Choose the Right Yuve Routine.
What is the bottom line for the best gut-health routine?
The best routine is the one that stays boring enough to repeat: fiber at meals, fermented foods most days, water with the fiber, movement after a meal, and sleep timing that does not drift wildly. Yuve Probiotic Gummies and Yuve Prebiotic Fiber Gummies can fit that pattern when you want vegan, plant-based, low-friction support, but they work best beside food habits, not instead of them. The right choice is the option that removes friction without replacing breakfast, plants, water, walking, or sleep. For most people, consistency beats complexity because the microbiome responds to repeated daily inputs over meaningful time periods most weeks. If you want a simple product path, start with the Yuve digestive health collection, then choose prebiotic fiber gummies, probiotic gummies, or both based on the use case you will actually repeat.