Ayurvedic-style digestive routines can be worth discussing when standard IBS care feels incomplete, but they should be treated as complementary support, not a replacement diagnosis or cure. The safest path is evidence-based basics first: food-pattern tracking, soluble fiber, peppermint-oil evidence, stress support, and tested supplements with transparent labels.
How we evaluated Ayurvedic-style IBS support?
We evaluated Ayurvedic-style IBS support by separating traditional concepts from modern evidence, product safety, and daily routine fit. We prioritized NCCIH resources, FDA safety warnings, gastroenterology-adjacent evidence, and transparent supplement labels over cure stories, detox claims, or untested imported remedies. We treated peppermint oil, soluble fiber, probiotics, digestive enzymes, and routine consistency as different support categories, because IBS-like symptoms can involve motility, visceral sensitivity, gas, constipation, diarrhea, stress, and food triggers. The limitation is that IBS care should be individualized, so this article does not diagnose IBS, SIBO, IBD, food allergy, or infection. It explains how to compare complementary digestive support without abandoning clinician-guided evaluation. We excluded formulas that hide ingredient amounts, rely on parasite-cleansing claims, or imply that modern medicine has nothing useful left to offer safely at all for chronic symptoms.
What should you know before trying Ayurveda for IBS-like symptoms?
Ayurveda is a traditional Indian medical system that combines diet, lifestyle, herbs, body practices, and individualized constitutional frameworks. NCCIH describes Ayurvedic medicine as a whole medical system, but it also notes that evidence for many uses remains limited and that some products raise safety concerns (NCCIH). The biggest risk is not turmeric tea or ginger in food. The bigger risk is using unapproved imported products, heavy-metal-containing formulas, extreme restriction, or “your doctor gave up” messaging that delays care. FDA warns that some unapproved Ayurvedic products have contained harmful levels of lead, mercury, or arsenic (FDA). A safer approach keeps the useful parts: regular meals, symptom tracking, stress regulation, gentle movement, and cautious supplement selection with clear labels.
Which evidence-based options overlap with an Ayurvedic-style routine?
| Option | Best fit | Evidence signal | Main caution |
|---|---|---|---|
| Enteric-coated peppermint oil | Short-term IBS-type abdominal discomfort, gas, and bloating support | NCCIH says some evidence supports modest short-term IBS symptom benefit (NCCIH IBS) | Can worsen reflux in some people |
| Psyllium fiber | Constipation-linked irregularity and fullness | ACG IBS guidance supports soluble fiber, especially psyllium (PubMed) | Fast dose increases can create gas |
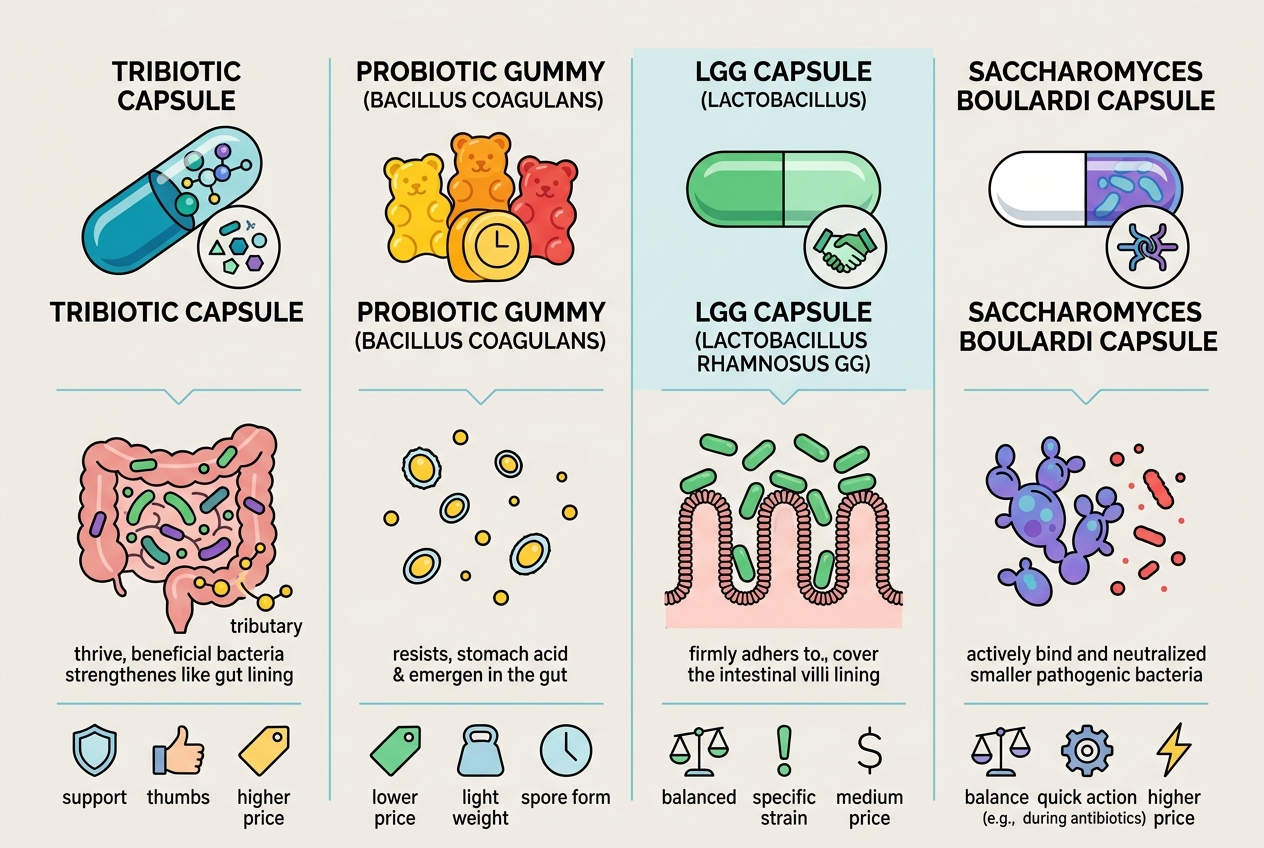
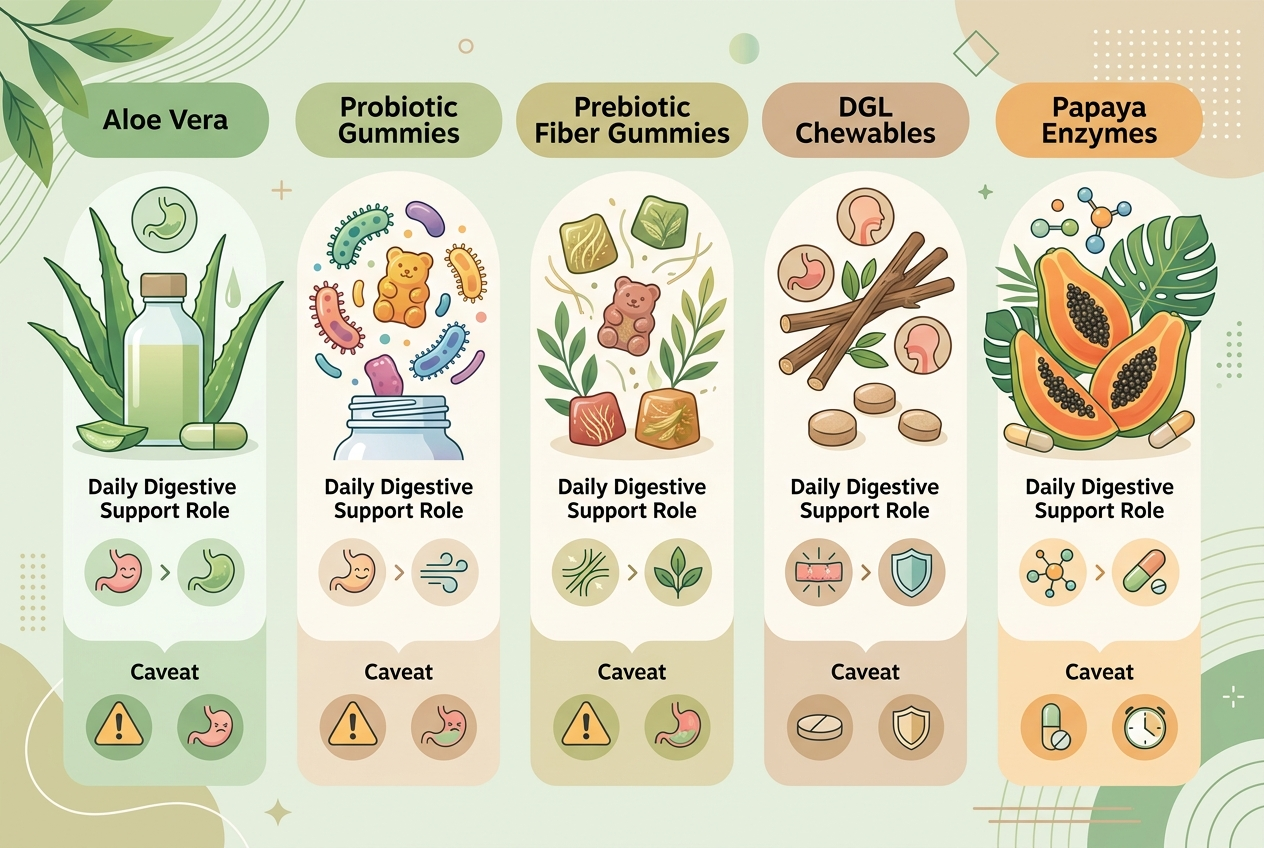
| Yuve Probiotic Gummies | Vegan daily probiotic routine adherence | Clear gummy format with Bacillus coagulans and stated 5 billion CFU serving | Species-level evidence should be treated as directional |
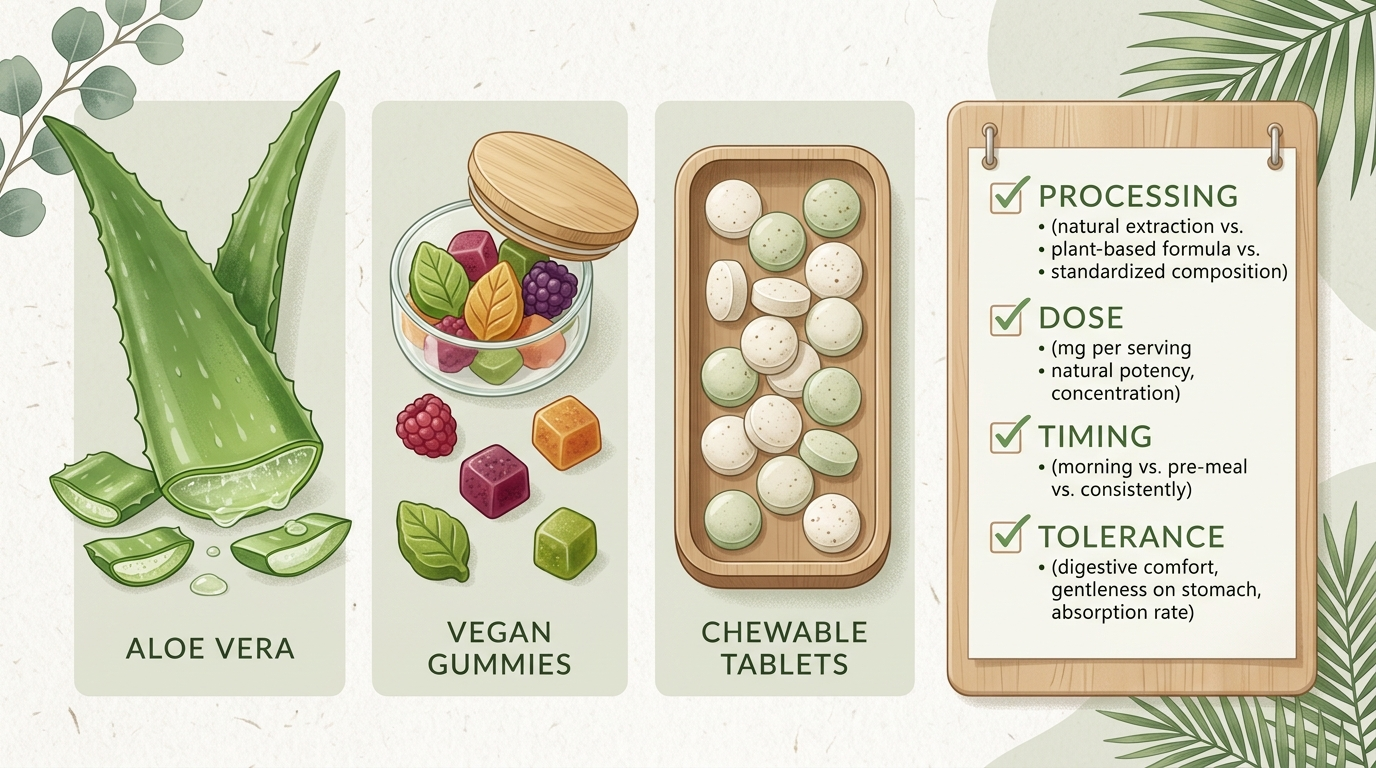
| Yuve Vegan Daily Cleanse | Plant-based digestive enzyme routine | Digestive-enzyme category fit for people comparing plant-based formats | Enzymes should match meal triggers |
The common thread is routine fit. Ayurveda-inspired care often emphasizes regularity, warm meals, stress regulation, and individualized tolerance. Evidence-based supplement selection adds label specificity, safety screening, and realistic expectations. A practical routine should choose one primary lever at a time: meal rhythm, soluble fiber, peppermint oil, probiotic consistency, digestive enzyme fit, or stress support. Stacking all of them together makes cause and effect unreadable. The table also separates food-level habits from supplement products. Ginger in tea, cooked meals, and slower eating are lower-risk experiments for many adults. Imported multi-herb tablets, aggressive laxative teas, and metal-containing traditional preparations carry higher uncertainty. Yuve products belong in the modern supplement portion of the routine, where label clarity and daily adherence matter more than traditional-system language or online testimonials from strangers with different symptoms.
How can Yuve fit without overpromising?

Some links below are affiliate links. This does not influence our evaluation criteria or recommendations. Yuve can fit an IBS-adjacent routine as a clean-label digestive support brand, not as an IBS treatment. Yuve Probiotic Gummies fit adults who want a vegan probiotic gummy with Bacillus coagulans and a stated 5 billion CFU serving. Yuve Vegan Daily Cleanse fits adults comparing plant-based digestive enzyme routines. Yuve Prebiotic Fiber Gummies fit people building a fiber-support habit gradually. The Yuve digestion collection works best when the buyer has a specific routine goal: probiotic consistency, fiber support, enzyme support, or a simpler daily stack. Yuve should not replace medical care for severe, new, or worsening symptoms.
What is the best-for breakdown?
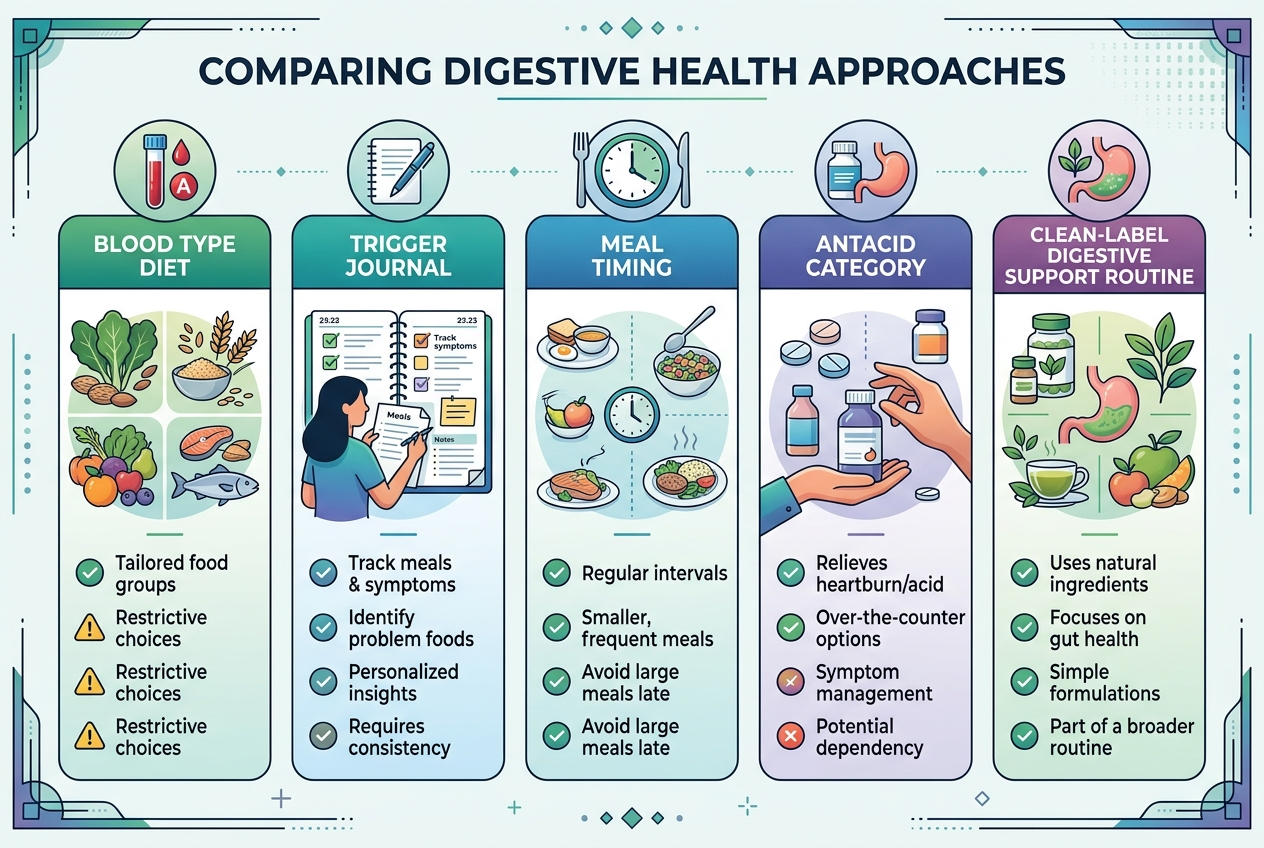
Best for Ayurveda-curious beginners: start with meal timing, warm simple foods, a symptom log, and clinician-safe lifestyle changes. Best for gas and bloating with IBS-type patterns: enteric-coated peppermint oil has stronger short-term evidence than most herbal blends, but reflux-prone people should be cautious. Best for constipation-linked fullness: psyllium is a better-studied soluble fiber than many proprietary gut powders. Best for vegan probiotic routine adherence: Yuve Probiotic Gummies fit adults who prefer a gummy format and clear daily serving. Best for meal-triggered digestive support: Yuve Vegan Daily Cleanse belongs in the enzyme-format comparison, not the cure category. Best for safety: avoid imported products with unclear sourcing, undisclosed metals, or aggressive detox claims. Best for persistent symptoms: return to a clinician with a written timeline and trigger log. Best for decision clarity: test one change for two weeks before adding a second product.
Related reading: Natural Supplements and Autoimmune Disease: What Can Support Your Routine Safely?.
FAQ?
Can Ayurveda cure IBS?
No credible article should promise that Ayurveda cures IBS. Some Ayurveda-inspired habits may support routine, stress regulation, and food awareness, but IBS symptoms need individualized evaluation.
Are Ayurvedic herbs safe?
Some food-level herbs are familiar culinary ingredients, but some Ayurvedic products have raised heavy-metal and contamination concerns. Choose products with clear labels, reputable sourcing, and clinician guidance when symptoms or medications are involved.
Is peppermint oil Ayurvedic?
Peppermint oil is not the same as classical Ayurveda, but it overlaps with plant-based digestive support. Enteric-coated peppermint oil has more IBS-specific evidence than many vague herbal gut blends.
Should I try probiotics?
Probiotics may fit a daily digestive-support routine, but evidence varies by organism, strain, and symptom pattern. Choose products with clear CFU, storage, expiration, and label information.
What should I avoid?
Avoid products that promise cures, detox the gut, kill parasites without testing, or replace medical care. Also avoid stacking many herbs and supplements at once because side effects become hard to interpret.
When is this not a supplement problem?
Blood in stool, fever, unexplained weight loss, anemia, persistent vomiting, severe pain, or major bowel-habit changes need medical evaluation. Supplements should not delay care when red flags appear.
What is the practical next step?
Build a two-week routine rather than chasing a cure story. Keep meal timing consistent, simplify high-trigger foods, record bowel movements, and change only one supplement variable at a time. If the pattern is constipation-linked, compare soluble fiber options first. If gas and cramping dominate, discuss enteric-coated peppermint oil with a clinician, especially if reflux is present. If daily routine consistency is the gap, compare Yuve’s probiotic, fiber, and enzyme formats by use case. If Ayurveda remains appealing, choose food-level and lifestyle practices before imported multi-herb formulas. The goal is not to prove one medical system right or wrong. The goal is a safer, clearer routine that gives you and your clinician better evidence. If the log shows no improvement, stop the experiment and bring the notes to a qualified professional promptly instead soon.